Pulmonary Medicine Blog By Dr Deepu
CT findings in bronchiectasis include the
following:
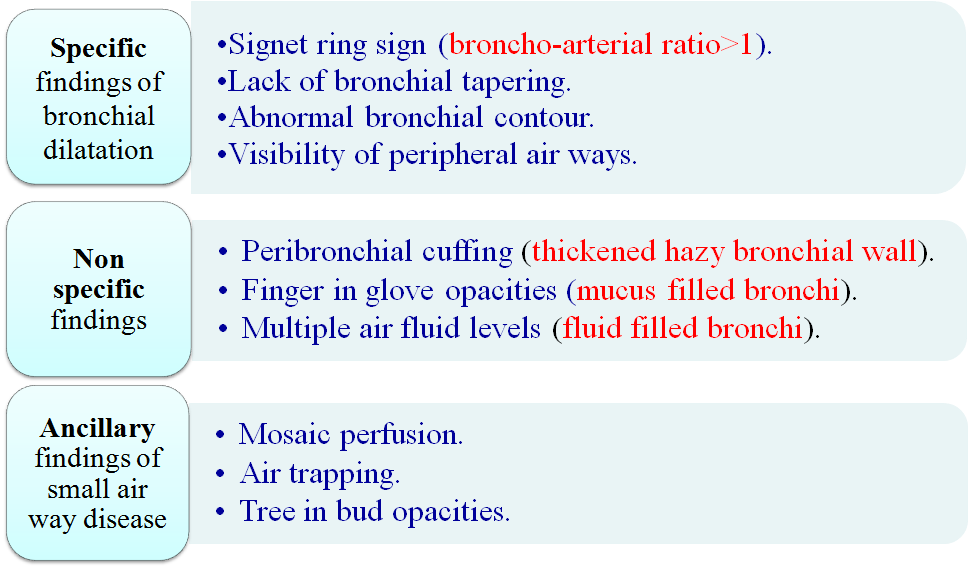
· Let me first describe the specific findings in the bronchiectasis
Has parallel tram track lines, or
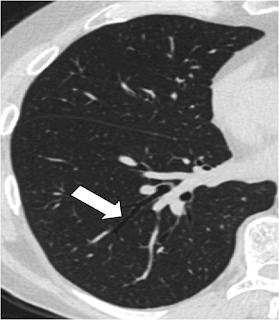
It may have a signet-ring appearance,
Let me make it more clearer, it is composed of a dilated bronchus cut in a horizontal section representing the golden ring; with an adjacent pulmonary artery representing the stone of the Ring. Take a look at the signet ring to get the idea.
· The diameter of the bronchus lumen is normally 1-1.5 times that of the adjacent vessel; a diameter greater than 1.5 times that of the adjacent vessel suggests bronchiectasis. Let us correlate it in the CT scan
Second Sign is lack of bronchial tapering, Normally as we move to the peripheral parts of the HRCT, the Bronchus should start tapering, as the diameter of the bronchus progressively decreases, whereas in the patients with bronchiectasis this tapering is not seen as the bronchial wall is destroyed and dilated , see the images below
 |
| NORMAL BRONCHIAL TAPERING |
 |
| LACK OF BRONCHIAL TAPERING |
We can also see the abnormal bronchial contour due to the tractional forces applied by the fibrosed and diseased lungs
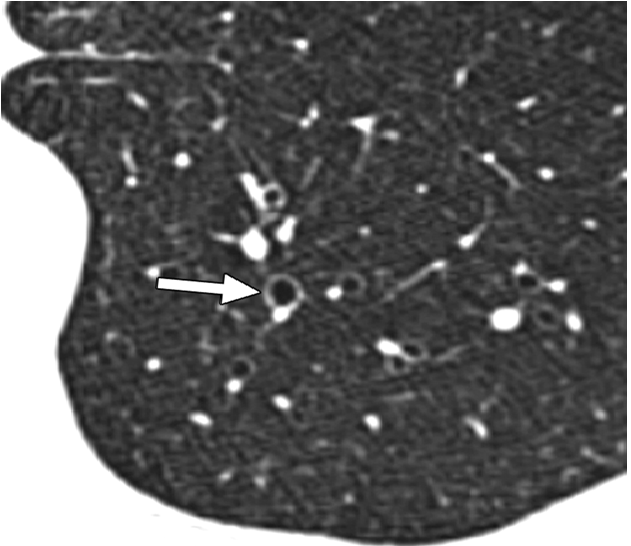
Visibility of peripheral airways within 1 cm of the pleura
Normally airways are not seen upto 1 cm from the pleura but with bronchiectasis we may be able to see the dilated peripheral airways
 |
| ARROWS POINTING TO THE DILATED PERIPHERAL AIRWAYS WITHIN 1 CM OF PLEURA |
Its time to describe the non specific findings in the bronchiectasis
•Peribronchial cuffing (thickened hazy bronchial wall).
•Finger in glove opacities
(mucus filled bronchi).
•Multiple air fluid levels
(fluid filled bronchi).
Peripheral cuffing- here we have a thickened bronchial wall due to constant underlying inflammatory process in the bronchial wall
 |
| PATIENT WITH LONG STANDING ABPA SHOWING BRONCHIECTASIS IN THE RIGHT LUNG, WITH BRONCHIAL WALL THICKENING |
Finger in glove opacities( Mucus filled bronchi)
mucus plugging of the bronchus causes bronchus to appear as a gloved hand
let us see how it appears in the CT Scan
Does this look like a gloved finger???
Next sign is multiple air fluid levels
tThis occurs due to the dilated bronchus and the fluid collected in the dilated bronchus.
Along with these specific and non specific finding we will be able to see few ancillary findings associated with bronchiectasis
•Mosaic perfusion.
•Air trapping.
•Tree in bud opacities.
Mosaic Perfusion
It occurs due to areas alternating areas of normal lung and trapped air in the lungs
Air Trapping, to see air trapping specifically ask for expiratory film, the air gets trapped in the blocked small airways causing dark areas, whereas the air is squeezed out from normal lung.
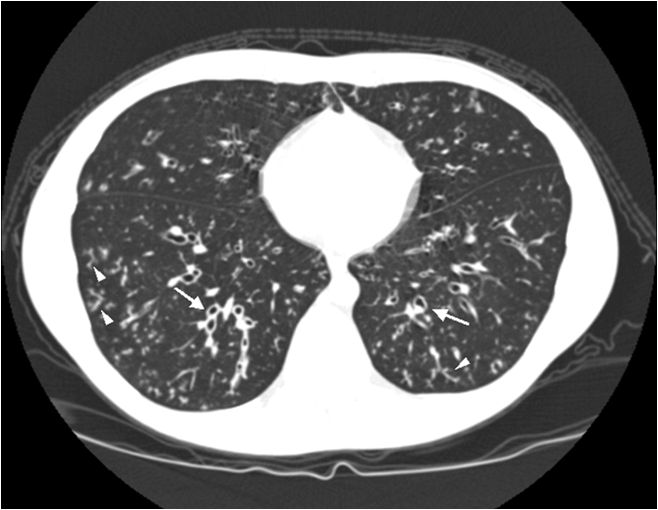
Tree in Bud Appearance-
occurs due to active infection, study the image and find tree in bud, I have marked it in 2nd image
 |
| Image shows bronchiectasis and tree in Bud |
tIf you liked the post please comment , comments activates the search engine, Thanks
Suggested Reading
My Next post will be on "SOLITARY PULMONARY NODULE"


































.jpg)
.jpg)
.jpg)



.jpg)
.png)
.png)

.png)